Health
Coverage Worries Persist Amid Relief Over Health Care Ruling

Affordable Care Act participant Kim Jones poses for a photo in her home in Wake Forest, N.C., Thursday, June 25, 2015. Jones said the Affordable Care Act has been a blessing to her who could not have otherwise afforded the medical care she has received during treatment for a tumor on her brain. The Supreme Court decided Thursday to uphold the Affordable Care Act subsidies. (AP Photo/Gerry Broome)
CARLA K. JOHNSON, Associated Press
CHICAGO (AP) — Throughout the country, relief was the dominant emotion among consumers who get help from the government to lower their health insurance costs following Thursday’s Supreme Court ruling upholding the subsidies underpinning President Barack Obama’s health care overhaul.
Many consumers expressed somewhat conflicting views: They were happy their monthly premiums would continue to be affordable but exasperated by the coverage the policies purchased on the new health care exchanges provide.
“I don’t particularly care for Obama. I didn’t vote for him,” said Salt Lake City resident Paige Preece, whose subsidy allows her to buy insurance for $137 a month. “But, honestly, if it weren’t for this, I would be absolutely lost.”
The court’s 6-3 ruling upheld the federal financial assistance to millions of low- and middle-income Americans to help pay for insurance premiums regardless of where they live. An estimated 6.4 million people in the 34 states that used the federal health care exchange were at risk of losing the subsidies because their home states did not set up their own insurance exchanges.
The case turned on just a few words in the mammoth Affordable Care Act that suggested the federal subsidies could go only to consumers in states that operated their own health insurance marketplaces. Consumers in those states or in ones that fell back on the federal exchange when their own exchanges faltered were not affected by the case.
“Congress passed the Affordable Care Act to improve health insurance markets, not to destroy them,” Chief Justice John Roberts declared in the majority opinion.
Polls taken before Thursday’s ruling suggested that most Americans wanted the court to uphold the subsidies. In an April Associated Press-GfK poll, 56 percent preferred that the court rule in favor of the Obama administration, while 39 percent wanted the court to rule for the other side.
Lydia DeJesus, who helps people sign up for coverage in Dickinson, North Dakota, said she has noted that division among consumers concerning the health care law, even among those receiving significant subsidies that make their policies more affordable.
“There are people who have services who never had services,” she said. “But there are people who were forced to have insurance and really don’t consider it affordable. Some people have told us they’d rather pay the fine as opposed to having health insurance.”
In Gresham, Oregon, Anna Mar, 28, said she is still no fan of what she calls “Obamacare.” She is a stay-at-home mom with two young boys. Her husband works in construction.
“The plan hardly covers anything, so I avoid going to the doctor,” Mar said. “I love the idea of everyone having health care, but it’s not affordable for us.”
For herself, Mar bought the cheapest plan on the exchange she could find: $134 a month, with a high deductible and high co-pays. Her government subsidy is $40. The couple’s children qualify for Medicaid, the state-federal health program for those with lower incomes.
Other consumers said they were grateful for the health care reforms and for Thursday’s ruling allowing the subsidies to continue.
Kim Jones, a substitute teacher in Wake Forest, North Carolina, said she once used the emergency room for her care. With the health insurance plan she purchased on the federal exchange, she now can afford follow-up treatment after surgery last summer to remove a brain tumor.
Jones, 60, said she was without health insurance for about a decade because of the part-time jobs she took to allow her to care for an elderly parent. Her current coverage costs her about $27 a month, after the government subsidy of more than $500. She continues to take medication and had worried about losing coverage.
“I know it helped so many people, and a lot of folks like myself who had fallen through the cracks were finally getting some kind of help with health issues,” Jones said after the ruling.
In Norman, Oklahoma, Kelli Nicole Smith, a 26-year-old baker who earns $11 an hour at a candy shop, said she was relieved to learn she would still receive the $99 monthly subsidy that she used to purchase a health plan. Without it, Smith said she probably would have considered buying less healthy food or downgrading her mobile phone plan.
“I would have choices, but they wouldn’t be comfortable,” said Smith, who ends up paying about $60 a month for a plan with relatively high co-pays, including $500 for an emergency room visit. “Or I would have to consider finding a job that maybe pays more that I don’t really want to do.”
Advocates such as Walter Davis of the Tennessee Health Care Campaign, used the Supreme Court decision to urge lawmakers in Tennessee to increase Medicaid access, an expansion that was made optional by an earlier Supreme Court ruling.
“Tennessee has failed to expand Medicaid and is falling further behind, leaving thousands of people unnecessarily uninsured and without access to affordable health coverage,” he said in a written statement. “Now Tennessee policymakers should recognize health reform is working, abandon efforts to undermine it, and instead take advantage of the opportunities that health reform offers to improve lives.”
Those with medical issues took the most comfort in the Supreme Court’s ruling and Obama’s assertion afterward that “the Affordable Care Act is here to stay.”
“I’m starting to cry just talking about it,” said Susan Halpern, a 55-year-old breast cancer survivor from Columbus, Ohio, who immediately posted the news to Facebook.
With an irregular income as a freelance contractor, she said the subsidy makes a huge difference. Without it, she said the only way she could continue to pay the premium would be to drain her retirement savings.
“This has saved my ability to retire someday,” Halpern said. “I know tens of thousands of Americans were looking at it the same way.”
___
Associated Press writers Emery P. Dalesio in Raleigh, North Carolina; Travis Loller in Nashville, Tennessee; James MacPherson in Bismarck, North Dakota; Sean Murphy in Oklahoma City; Michelle L. Price in Salt Lake City; and John Seewer in Toledo, Ohio, contributed to this report.
Copyright 2015 The Associated Press. All rights reserved. This material may not be published, broadcast, rewritten or redistributed.












Activism
Essay: Intentional Self Care and Community Connections Can Improve Our Wellbeing
At the deepest and also most expansive level of reality, we are all part of the same being, our bodies made from the minerals of the earth, our spirits infused by the spiritual breath that animates the universe. Willingness to move more deeply into fear and pain is the first step toward moving into a larger consciousness. Willingness to move beyond the delusion of our separateness can show us new ways of working and living together.

By Dr. Lorraine Bonner, Special to California Black Media Partners
I went to a medical school that was steeped in the principles of classical Western medicine. However, I also learned mindfulness meditation during that time, which opened me to the multifaceted relationship between illnesses and the interconnecting environmental, mental and emotional realities that can impact an individual’s health.
Therefore, when I began to practice medicine, I also pursued training in hypnosis, relaxation techniques, meditation, and guided imagery, to bring a mind-body focus to my work in medical care and prevention.
The people I saw in my practice had a mix of problems, including high blood pressure, diabetes, and a variety of pain issues. I taught almost everyone relaxation breathing and made some general relaxation tapes. To anyone willing, I offered guided imagery.
“My work embraced an approach to wellness I call “Liberatory Health” — one that not only addresses the treatment and management of disease symptoms but also seeks to dismantle the conditions that make people sick in the first place.”
From my perspective, illness is only the outermost manifestation of our efforts to cope, often fueled by addictions such as sugar, tobacco, or alcohol, shackled by an individualistic cult belief that we have only ourselves to blame for our suffering.
At the deepest and also most expansive level of reality, we are all part of the same being, our bodies made from the minerals of the earth, our spirits infused by the spiritual breath that animates the universe. Willingness to move more deeply into fear and pain is the first step toward moving into a larger consciousness. Willingness to move beyond the delusion of our separateness can show us new ways of working and living together.
To put these ideas into practical form, I would quote the immortal Mr. Rogers: “Find the helpers.” There are already people in every community working for liberation. Some of them are running for office, others are giving food to those who need it. Some are volunteering in schools, libraries or hospitals. Some are studying liberation movements, or are working in urban or community gardens, or learning to practice restorative and transformative justice, or creating liberation art, music, dance, theater or writing. Some are mentoring high schoolers or apprenticing young people in a trade. There are many places where compassionate humans are finding other humans and working together for a better world.
A more compassionate world is possible, one in which we will all enjoy better health. Creating it will make us healthier, too.
In community, we are strong. Recognizing denial and overcoming the fragmenting effects of spiritual disorder offer us a path to liberation and true health.
Good health and well-being are the collective rights of all people!
About the Author
Dr. Lorraine Bonner is a retired physician. She is also a sculptor who works in clay, exploring issues of trust, trustworthiness and exploitation, as well as visions of a better world.
Activism
Prescribing Prevention: Doctors Turn to Lifestyle, Herbs and Veggies to Protect Against Chronic Illness in Black Californians

By Charlene Muhammad, California Black Media
Leibo Glover received his diabetes diagnosis at the same time he found out he needed a below-the-knee amputation.
“Minor,” thought the 63-year-old.
Glover had been self-medicating a toe injury before seeing the doctor.
But while driving from South Los Angeles to Miami on a family trip, an infection set in.
“I had it but didn’t know,” said Glover. “I was just going to come back to California, but they told me if I had left, I would have come home as a corpse,” Glover told California Black Media (CBM).
A majority of the nearly 3.5 million Californians diagnosed with diabetes have preventable Type 2 diabetes, according to researchers at the UCLA Center for Health Policy Research.
In 2023, diabetes was diagnosed in 1 in 6 adults with the lowest incomes (16.7% at 0–99% of the federal poverty line), compared to 1 in 11 adults with the highest incomes (8.9% at 300% or more of the federal poverty line). Age is a factor, too: more than 1 in 5 older adults age 65 and over (22.3%) had diabetes, about twice the rate of adults age 18–64 (8.6%).
Another study by Health Economics and Evaluation Research (HEER) mapped patients with diabetes in California who had amputations. Researchers found that patients living in low-income ZIP codes were far more likely to have had lower-limb amputations than those in higher-income ZIP codes, essentially identifying amputation “hot spots.”

At the time of Glover’s 2018 diagnosis, he was experiencing housing instability and going through financial hardships. Now, he has more stable housing and he has improved his health through lifestyle changes like eating healthier and getting more sleep.
“If the equipment is right, I can stand on my leg for hours. I can actually run, jump, dance and all of that,” said Glover, who got his diabetes under control, in part, by avoiding carbohydrates and sugars.
As chronic illnesses continue to disproportionately impact Black Californians — often leading to preventable amputations and premature deaths — a growing number of doctors and advocates are expanding their care from just treatment to including prevention. From promoting diet and lifestyle changes to cultivating community farms focused on prevention and wellness like Dr. Bill Releford’s Bloom Ranch in Acton.
Releford, a podiatrist based in Los Angeles started the 250-acre Bloom Ranch in 2023 as part of his strategy for preventive care.
“This is my assignment,” said Releford.
“Bloom Ranch has been a perfect backdrop for me to be creative and to find avant-garde ways to make fresh fruits and vegetables more accessible to food deserts in Los Angeles County,” he stated.
California produces nearly half of the nation’s fruits and vegetables, yet more than 1 in 5 Californians — about 8.8 million people — currently struggle with food insecurity, according to the California Association of Food Banks.
“Studies have shown that 75% of amputations are preventable. And African Americans have the highest amputation rate in the nation,” Releford said.
As such, Releford continued, the mortality rate associated with high-level amputation is 50%, which means “if we had 10 people that all had high level amputations, five of those would be deceased in three years.”

Monday, June 28, 2025. Leibo Glover at his home in Los Angeles, California. The security professional’s leg was amputated below the knee.
Releford’s ranch is the largest Black-owned farm in L.A. County. He plans to partner with UCLA and the Charles R. Drew University of Medicine and Science to develop prescriptive vegetable boxes.
“Certain vegetables and herbs can lower blood pressure naturally, like beets, turnips, dill, basil, garlic and others,” said Releford.
“Hopefully, this will inspire other farmers to take this model and replicate it across other urban areas,” Releford added.
“A lot of studies have shown that gardening has so many health benefits – being in the sun, Vitamin D,” said Releford. “The dirt has a lot of microbes that are good for your immune system. Studies have shown that people who work in the dirt have strong immune systems.”
Gardening can potentially decrease the risk of dementia, enhance cognition, reduce stress, and boost immunity, indicates research by Genoa Barrow of the University of Southern California Center for Health Journalism as part of the 2024 Ethnic Media Collaborative, Healing California.
During a recent picturesque day at Bloom Ranch, families, school children, farmers and members of The Ultimate Book Club 1998, founded by Alina Anderson, sampled and purchased fresh produce while taking photographs.
“This is huge. “All of us have families that could use this information,” said Anderson.
Doctors like Releford, who are committed to tackling the most chronic diseases impacting all their patients utilize peer-to-peer support programs with self-management training led by individuals living with chronic conditions to provide role models and support for patients, according to a recent study by the California Health Care Foundation.
“The unifying feature of these programs is that they seek to build on the strengths, knowledge, and experience that peers can offer,” the report states.
Liz Helms, CEO of the California Chronic Care Coalition, addressed state-backed prevention policy and initiatives.
“It’s in horrible shape. It needs to get so much better, especially in underserved areas, where the Black population has a whole set of different needs,” she said.
Helms, who started advocacy after being denied access to care in the early 1990s, applauded new developments in telehealth. The opportunity to choose between visiting a doctor’s office or placing a phone call makes a difference, especially if there are transportation or distance issues, or if one is too sick, she said.
Fear is one thing people, especially in the Black community, must overcome, emphasized Helms.
“I had to get over my fear of going to the doctor, of not speaking up,” continued Helms, urging patients to “understand the baseline” of their health.
“Don’t let anyone stigmatize you or tell you that you’re not good enough to get care or look down on you. Everyone has a right to good, quality, affordable, timely health care,” said Helms.
To engage Bloom Ranch for preventive care focused on wellbeing and healthy living, call (323) 388-4828 or sign up at Bloomranchofacton.com
Activism
A West Coast CDC? California Partners With Oregon, Washington and Hawaii to Form Regional Health Alliance
“President Trump’s mass firing of CDC doctors and scientists — and his blatant politicization of the agency — is a direct assault on the health and safety of the American people. California, Oregon, and Washington will not allow the people of our states to be put at risk,” said Governors Gavin Newsom, Tina Kotek, and Bob Ferguson in a joint statement.

By Bo Tefu, California Black Media
California, Oregon, and Washington have launched the West Coast Health Alliance, a regional initiative to provide unified, science-based guidance on immunizations and other public health policies. The alliance was created in response to federal actions that have undermined the independence of the Centers for Disease Control (CDC) and raised concerns about the politicization of science.
The alliance aims to ensure residents receive credible, evidence-based recommendations, free from political interference.
“President Trump’s mass firing of CDC doctors and scientists — and his blatant politicization of the agency — is a direct assault on the health and safety of the American people. California, Oregon, and Washington will not allow the people of our states to be put at risk,” said Governors Gavin Newsom, Tina Kotek, and Bob Ferguson in a joint statement.
State health leaders emphasized the importance of transparency and evidence-based communication.
California Department of Public Health Director Erica Pan said, “The dismantling of public health and dismissal of experienced and respected health leaders and advisors, along with the lack of using science, data, and evidence to improve our nation’s health are placing lives at risk.”
Oregon Health Authority Director Sejal Hathi backed the coalition saying, “Our communities deserve clear and transparent communication about vaccines — communication grounded in science, not ideology.” Washington State Secretary of Health Dennis Worsham noted, “Public health at its core is about prevention — preventing illness, preventing the spread of disease, and preventing early, avoidable deaths.”
Hawaii has joined the alliance, expanding the partnership to four states. “Hawaii is proud to stand with our West Coast partners to ensure public health decisions are grounded in science, not politics,” said Gov. Josh Green.
The alliance states will coordinate health guidelines using trusted national medical organizations, aligning immunization recommendations and public health strategies while respecting tribal sovereignty. Shared principles to strengthen public confidence in vaccines and other health measures will be finalized in the coming weeks.


WORK FROM HOME
Home-based business with potential monthly income of $10K+ per month. A proven training system and website provided to maximize business effectiveness. Perfect job to earn side and primary income. Contact Lynne for more details: Lynne4npusa@gmail.com 800-334-0540
![]()

Oakland Post: Week of December 10 – 16, 2025

Seth Curry Makes Impressive Debut with the Golden State Warriors

LIHEAP Funds Released After Weeks of Delay as States and the District Rush to Protect Households from the Cold

Seven Steps to Help Your Child Build Meaningful Connections

Seven Steps to Help Your Child Build Meaningful Connections

Teens Reject Today’s News as Trump Intensifies His Assault on the Press

Thanksgiving Celebrated Across the Tri-State

Breaking the Silence: Black Veterans Speak Out on PTSD and the Path to Recovery

Trinidad and Tobago – Prime Minister Confirms U.S. Marines Working on Tobago Radar System

‘Tis the Season: Festive Holiday Pop-ups Happening Around Atlanta

IN MEMORIAM: Mardelle Walker, 101

Oakland Post: Week of November 26 – December 2, 2025

‘Targeted’ Shooting of Two National Guardsmen Blocks From the White House

Meet Roxanne Brown, The First African American And The First Woman President Of The United Steelworkers

Tax Refunds Expected to Rise by About $1,000 Next Year

Oakland Post: Week of October 29 – November 4, 2025

Oakland Post: Week of November 12 – 18, 2025

Oakland Post: Week of November 5 – 11, 2025

IN MEMORIAM: William ‘Bill’ Patterson, 94

How Charles R. Drew University Navigated More Than $20 Million in Fed Cuts – Still Prioritizing Students and Community Health

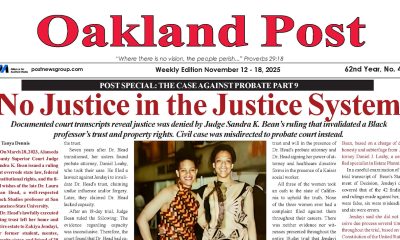
No Justice in the Justice System

Beyoncé and Jay-Z make rare public appearance with Lewis Hamilton at Las Vegas Grand Prix

Lewis Hamilton set to start LAST in Saturday Night’s Las Vegas Grand Prix

Oakland Post: Week of November 19 – 25, 2025

Protecting Pedophiles: The GOP’s Warped Crusade Against Its Own Lies

The Perfumed Hand of Hypocrisy: Trump Hosted Former Terror Suspect While America Condemns a Muslim Mayor

Trump’s Death Threat Rhetoric Sends Nation into Crisis
LIHEAP Funds Released After Weeks of Delay as States and the District Rush to Protect Households from the Cold
Seth Curry Makes Impressive Debut with the Golden State Warriors
Thanksgiving Celebrated Across the Tri-State

Hyundai Ioniq 5 Parking, Safety, and 360 View #shorts

2025 Ioniq 5 New Wiper & Powerful Performance! #shorts

Electric SUV Range: Is 259 Miles Enough? #shorts

EV Charging: How Fast Can You Charge an Electric Vehicle? #shorts

Biometric Cooling… Messaging Seats…Come on! 2025 Infiniti QX80 Autograph 4WD

Charged Up: Witness the Magic of a Fully Electric Car! #shorts

Range Rover Sport PHEV Included…: See What’s Inside This Luxury SUV! #shorts

Invisible Hood View: Perfect Parking with X-Ray Vision! #shorts

AI Is Reshaping Black Healthcare: Promise, Peril, and the Push for Improved Results in California

ESSAY: Technology and Medicine, a Primary Care Point of View

Sanctuary Cities

The RESISTANCE – FREEDOM NOW

STATE OF THE PEOPLE: Freddie

ECONOMIC BOYCOTT DAY!!!!!

I told You So
-
 Activism4 weeks ago
Activism4 weeks agoOakland Post: Week of November 12 – 18, 2025
-
 Activism3 weeks ago
Activism3 weeks agoIN MEMORIAM: William ‘Bill’ Patterson, 94
-
 Activism4 weeks ago
Activism4 weeks agoHow Charles R. Drew University Navigated More Than $20 Million in Fed Cuts – Still Prioritizing Students and Community Health
-
 Bay Area4 weeks ago
Bay Area4 weeks agoNo Justice in the Justice System
-
 #NNPA BlackPress3 weeks ago
#NNPA BlackPress3 weeks agoBeyoncé and Jay-Z make rare public appearance with Lewis Hamilton at Las Vegas Grand Prix
-
 #NNPA BlackPress3 weeks ago
#NNPA BlackPress3 weeks agoLewis Hamilton set to start LAST in Saturday Night’s Las Vegas Grand Prix
-
 Activism3 weeks ago
Activism3 weeks agoOakland Post: Week of November 19 – 25, 2025
-
 #NNPA BlackPress4 weeks ago
#NNPA BlackPress4 weeks agoThe Perfumed Hand of Hypocrisy: Trump Hosted Former Terror Suspect While America Condemns a Muslim Mayor